
By Dr. Sumitra Gantayet
MBBS, DNB (General Surgery), DNB (Plastic Surgery), BEOFFA Fellow
Consultant Reconstructive & Plastic Surgeon | Divyam Reconstructive Diabetic Foot Care (RDFC), Visakhapatnam
Member: Association of Plastic Surgeons of India | Indian Society for Surgery of the Hand | Diabetic Foot Society of India
In my years of practice as a reconstructive plastic surgeon, one pattern repeats itself with heartbreaking frequency: patients arrive at our clinic in Visakhapatnam with a wound that has been quietly worsening for weeks — sometimes months. By the time they reach us, what began as a small sore on the sole has evolved into a deep infection involving bone, threatening the entire limb.
I share this not to alarm you, but because the most powerful tool I have — as both a surgeon and a doctor committed to limb preservation — is an informed patient.
Andhra Pradesh carries one of India’s heaviest diabetes burdens. Research consistently confirms that severe diabetic foot infections remain among the leading drivers of lower-limb amputation worldwide — a reality I witness in our clinic and in Vizag’s hospitals daily. Peripheral neuropathy quietly destroys sensation. Poor circulation starves tissue of the oxygen it needs to heal. Patients often don’t notice a wound until infection has already taken hold.
The psychological weight is equally serious. Chronic, non-healing ulcers trap patients in cycles of pain, immobility, and fear — fear that the next hospital visit ends with losing a limb. That fear is understandable. But in the vast majority of cases, it is preventable.
That is precisely why advanced diabetic foot reconstructive surgery — and the multidisciplinary team behind it — matters so profoundly here in Vizag. There is a genuine window of opportunity, often measured in days rather than weeks, where skilled intervention can preserve limbs that amputation would otherwise claim.
What Type of Doctor Treats Diabetic Foot? Navigating the Specialist Landscape
One of the most common questions I hear from patients and their families is simply: who do I call first? It is a question that matters more than most people realise — because choosing the right specialist, or the right team, can genuinely be the difference between keeping and losing a limb.
Podiatrists, Vascular Surgeons, and Plastic Surgeons: Different Roles, One Goal
In my experience working within multidisciplinary diabetic foot teams, three core specialties each address a distinct layer of this condition:
- Podiatrists manage wound care, offloading, nail pathology, and early-stage ulcers — the first line of defence for many patients.
- Vascular surgeons restore blood flow to the foot through procedures like angioplasty or bypass — absolutely critical when poor circulation is preventing healing, which I see frequently in our North Coastal Andhra patient population.
- Plastic and reconstructive surgeons — my own specialty — handle complex tissue reconstruction when wounds are too deep, too large, or too poorly perfused to close on their own.
No single specialist can manage every layer of a severe diabetic foot case. In my practice at Divyam Cosmetic & Plastic Surgery, Visakhapatnam, I work closely with endocrinologists, vascular specialists, and infectious disease consultants because the evidence — and my own clinical outcomes — confirm that a coordinated team consistently outperforms any single-practitioner approach.
Why a ‘Diabetic Foot Surgeon’ Is Often a Reconstructive Specialist
The term ‘diabetic foot surgeon’ is used loosely, but in advanced care settings — and in the context of my own fellowship training through the British European Orthopaedic Foot and Ankle Academy (BEOFFA) — it typically refers to a surgeon trained in reconstructive microsurgery. This means someone capable of not just cleaning a wound, but rebuilding the foot’s architecture: closing defects, restoring tissue coverage, and occasionally rewiring circulation at the microscopic level.
As a member of both the Diabetic Foot Society of India and the Association of Plastic Surgeons of India, I have seen how the field has evolved — and how far outcomes have improved when limb salvage is embedded within a true multidisciplinary framework.
KGH vs. Private Specialists: A Practical Note for Vizag Residents
Government Kidney & General Hospital (KGH) provides vital, accessible care and handles high patient volumes — and I respect the critical role it plays in our healthcare system. However, for complex cases requiring microsurgical reconstruction or advanced vascular intervention, dedicated private specialist centres in Visakhapatnam typically offer faster access to focused diabetic foot teams, modern imaging, and continuity of postoperative care.
The right choice depends on wound severity, urgency, and your individual circumstances — but knowing that world-class reconstructive options exist locally is the first step. The next question is understanding exactly what those surgical options can achieve.
Advanced Limb Salvage: The Power of Reconstructive Microsurgery in Vizag
Understanding who to see is only part of the picture. For many patients and families, the more pressing question is: what can modern surgery actually do once a wound has reached a critical stage? The answer, in my experience, is far more than most families realise — even in cases that have already been told elsewhere that amputation is inevitable.
What Is Diabetic Foot Reconstructive Surgery?
Diabetic foot reconstructive surgery is an umbrella term for procedures designed to repair tissue damage, restore blood flow, and preserve the limb when conventional wound care has failed. Rather than defaulting to amputation, we work to rebuild what infection and poor circulation have destroyed.
Clinical evidence comparing limb salvage against amputation consistently shows that preserved limbs correlate with better long-term mobility, lower mortality risk, and significantly reduced rehabilitation costs. From my own surgical practice, I can add something that statistics alone cannot convey: patients who keep their natural limb walk differently — with confidence, independence, and a quality of life that prosthetics, however advanced, cannot fully replicate.
Flap Surgery: Bringing Healthy Tissue to the Problem
When a wound will not close because the surrounding tissue is too damaged or too poorly perfused, we can relocate healthy tissue from elsewhere in the body. This is the science behind flap surgery — one of the most powerful tools in my reconstructive repertoire.
A ‘flap’ is a section of skin, fat, and sometimes muscle — moved with its own blood supply intact — that is repositioned over the wound site to provide a living biological cover. Local flaps use nearby tissue; free flaps harvest tissue from a distant donor site, such as the thigh or forearm. Free flaps are technically demanding and require microsurgical skill, but they allow us to cover even large, complex defects on the sole or heel — areas where tissue loss is otherwise catastrophic.
Microsurgery: Rebuilding Circulation at the Cellular Level
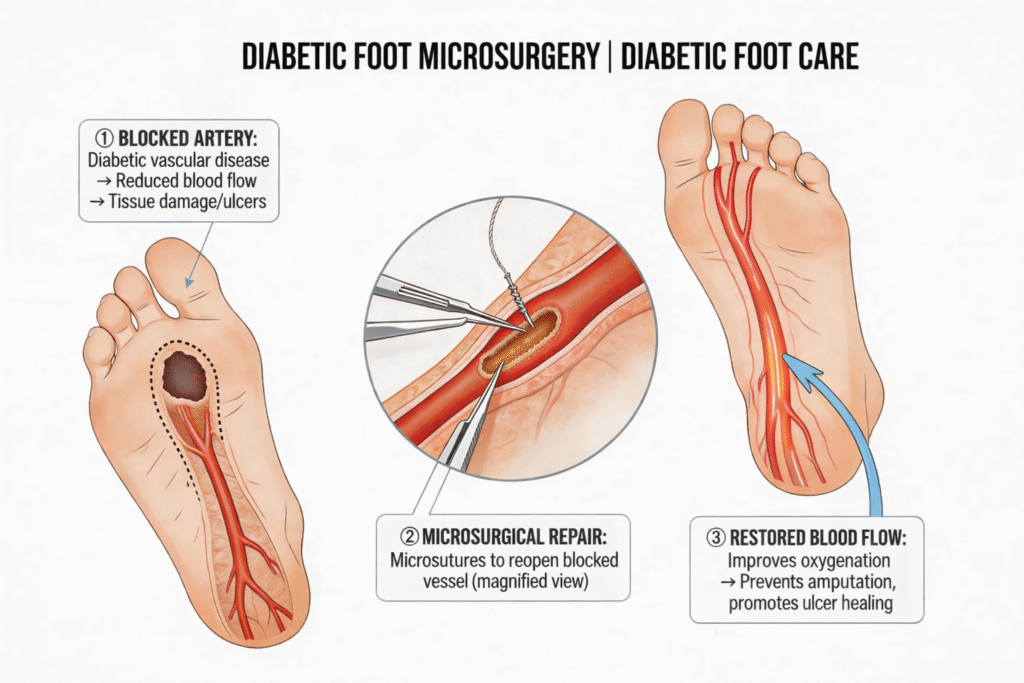
Microsurgery takes reconstruction a step further. Using specialised microscopes and instruments, we connect blood vessels as small as 1–2 millimetres in diameter — essentially rewiring circulation into a foot that had become ischaemic.
Published evidence on limb salvage in no-option critical limb ischaemia demonstrates that restoring even partial perfusion dramatically improves healing outcomes for wounds previously considered untreatable. Modern limb salvage centres report success rates exceeding 70–80% even in high-risk diabetic patients — outcomes that were unthinkable two decades ago. In my own practice, I approach every high-risk case with the conviction that the limb deserves every available surgical option before amputation is considered.
However, timing remains everything. These techniques perform best before irreversible tissue death sets in — which is why recognising the early warning stages of a diabetic foot ulcer is the most critical skill any patient or carer can have.
Recognising the Warning Signs: The 5 Stages and the ‘Rule of 50’
Most patients who eventually need microsurgical intervention arrive at our clinic far later than they should. I understand why — neuropathy silences pain, busy lives delay appointments, and wounds are easily dismissed when they don’t hurt. But the progression of a diabetic foot ulcer does not pause because life is busy.
Breaking Down the 5 Stages of a Diabetic Foot Ulcer (Wagner Classification)
In clinical practice, I grade diabetic foot wounds using the widely accepted Wagner Classification:
- Grade 0 — No open wound; intact skin with bony deformity or pressure callus. This is the stage where I can make the greatest difference — and where most patients do not yet see the need for a surgeon.
- Grade 1 — Superficial ulcer, no active infection. Still highly manageable with the right wound care and offloading.
- Grade 2 — Deep ulcer reaching tendon, joint capsule, or bone. Urgent specialist review required.
- Grade 3 — Deep ulcer with abscess, osteomyelitis, or joint infection. Surgical intervention almost always necessary.
- Grade 4 — Partial forefoot gangrene. Limb salvage still possible with aggressive intervention, but the window is narrow.
- Grade 5 — Whole foot gangrene. Major amputation is frequently unavoidable at this stage.
What I want every patient to understand: the transition from Grade 0 to Grade 3 can happen in days — particularly when neuropathy has already erased the pain signals that would otherwise bring someone to a clinic.
The ‘Rule of 50’ — A Clinical Benchmark Worth Knowing
The ‘Rule of 50’ is a sobering framework I often share with patients and their families to illustrate the stakes:
- Approximately 50% of diabetic foot ulcers become infected.
- 50% of infected ulcers lead to some form of amputation.
- Diabetic patients account for roughly 50% of all non-traumatic lower-limb amputations globally.
Each of those 50% figures represents a decision point — a moment where earlier specialist intervention would have changed the outcome. I have seen patients move through all three of those statistics unnecessarily, simply because the urgency was not communicated clearly enough at an earlier stage.
When a Callus Becomes a Surgical Emergency
A callus concealing a pressure ulcer beneath it is one of the most deceptive presentations I encounter. In a neuropathic diabetic foot, a callus over a bony prominence is a Grade 0 emergency — not a cosmetic nuisance to be addressed at the next convenient appointment.
For Indian patients specifically, the lifetime risk of developing a diabetic foot ulcer is estimated between 15–25% — a figure amplified by delayed diagnoses and inconsistent specialist follow-up. Recognising these stages early is what makes limb salvage a realistic, rather than theoretical, option.
Choosing a Specialist in Visakhapatnam: What to Look For
Not every clinic offering diabetic foot care is equipped to deliver true limb salvage outcomes. Over the years, I have received referrals from patients who had spent months at facilities without access to vascular imaging, microsurgical capability, or a proper multidisciplinary team. By the time they reached us, their options were significantly narrowed.
Here is what I would look for — as both a surgeon and as someone who would want this care for my own family.
Infrastructure That Matches the Complexity of the Condition
A dedicated diabetic foot clinic signals genuine multidisciplinary commitment — wound care nurses, vascular specialists, orthopaedic surgeons, and endocrinologists working under one roof. Without that integrated structure, care becomes fragmented. Look for:
- On-site vascular imaging (Doppler ultrasound, angiography access)
- Documented protocol for after-hours diabetic foot emergencies — because wound deterioration does not observe clinic hours
- A reconstructive surgeon with specific training in flap surgery and microsurgery for the foot
- A multidisciplinary case review process, where complex wounds are discussed collaboratively
Questions Every Patient Should Ask Their Surgeon
Before committing to a treatment plan, ask your diabetic foot surgeon these specific questions — and take note of how they respond:
- “What is your limb salvage rate for Stage 4 and Stage 5 wounds?”
- “What flap survival percentage do you achieve in free tissue transfers?”
- “Do you have a vascular interventionist available for revascularisation, if needed?”
A surgeon confident in their outcomes will answer these without hesitation. Vague responses or deflections are a red flag — not a sign of modesty.
Why Vizag Is Becoming a Regional Limb Salvage Hub
At Divyam RDFC Visakhapatnam, we regularly see patients travelling from Odisha, Srikakulam, and throughout North Coastal Andhra — choosing the additional journey over accepting an amputation-first approach closer to home. Visakhapatnam’s growing concentration of vascular surgeons, reconstructive microsurgeons, and advanced wound care infrastructure makes it one of the few genuine multidisciplinary limb preservation centres in eastern India — without requiring patients to travel to Chennai or Hyderabad.
That regional access, combined with the right specialist team, is something I feel a genuine professional responsibility to make available to every patient who walks through our doors.
Your Path to Walking Again: A Note from My Surgical Practice
I want to close with a statistic that I think about every time I enter the operating theatre: up to 85% of diabetes-related amputations are preventable with timely, specialist-led intervention.
That figure should fundamentally reframe how every diabetic patient thinks about a wound that ‘won’t heal.’ It is not bad luck. It is not inevitable. In the majority of cases, it is the result of a gap between the moment intervention was possible and the moment it was sought.
Patients who preserve their natural limb consistently report better long-term mobility, lower healthcare costs, and significantly higher quality of life compared to those who adapt to prosthetic alternatives. Walking naturally supports cardiovascular health, independence, and mental well-being in ways that are genuinely difficult to replicate.
The good news for residents of Vizag and the surrounding region: expert reconstructive diabetic foot care — including flap surgery, microsurgery, vascular assessment, and comprehensive postoperative support — is accessible right now, through our team at RDFC Visakhapatnam.
If you or someone you love has a diabetic foot wound that is not healing, please do not wait. Book a specialist consultation today.
Because in diabetic foot care, waiting is the one choice that consistently turns a treatable wound into an irreversible outcome.
About the Author
Dr. Sumitra Gantayet | MBBS, DNB (General Surgery), DNB (Plastic Surgery), BEOFFA Fellow
Dr. Sumitra Gantayet is a Consultant Reconstructive and Plastic Surgeon at Reconstructive Diabetic Foot Care (RDFC) Clinic, Visakhapatnam. She holds a BEOFFA Fellowship from the British European Orthopaedic Foot and Ankle Academy and is a member of the Association of Plastic Surgeons of India, Indian Society for Surgery of the Hand (ISSH), and the Diabetic Foot Society of India. Her clinical focus is advanced limb preservation, flap surgery, and microsurgical reconstruction for complex diabetic foot wounds.
Clinic: 2nd Floor, Coastal One, Plot No. 1, Balaji Nagar, Siripuram, Visakhapatnam 530003
Emergency: +91 88867 35004 (24/7)
FAQS
1. When should I see a specialist for a diabetic foot wound?
You should consult a specialist if a wound has not healed within 2–3 weeks, if there are signs of infection, bone exposure, or colour changes in the foot. In neuropathic patients, even a painless callus over a bony prominence warrants urgent review — it may conceal a deeper Grade 0 ulcer.
2. What is the ‘Rule of 50’ in diabetic foot care?
The Rule of 50 states that approximately 50% of diabetic foot ulcers become infected, 50% of infected ulcers lead to amputation, and diabetic patients account for roughly 50% of all non-traumatic lower-limb amputations globally. Each figure represents a decision point where earlier specialist intervention changes the outcome.