
If you or someone in your family is living with a wound that refuses to heal — particularly a diabetic foot ulcer — your doctor has almost certainly discussed debridement. But what exactly does it mean, and why does the specific method matter so much?
Wound debridement is the medical removal of dead, infected, or damaged tissue from a wound so that healthy tissue can heal. There are five main types of wound debridement: surgical (sharp), autolytic, enzymatic, mechanical, and biological. Each works differently and suits a different clinical situation. Choosing the wrong method — or delaying debridement altogether — can dramatically slow healing and increase the risk of serious infection.
At Divyam – RDFC (Reconstructive Diabetic Foot Care), Visakhapatnam, our specialist plastic surgeons conduct comprehensive wound assessments before recommending any debridement strategy. This guide explains every type in detail so you can understand your care plan and ask the right questions.
This article has been written with clinical input from Dr. Sumitra Gantayet, Consultant Reconstructive and Plastic Surgeon at RDFC Visakhapatnam. Dr. Gantayet holds qualifications including MBBS, DNB (General Surgery), DrNB Plastic Surgery, and a BEOFFA Fellowship (British European Orthopaedic Foot and Ankle Academy), and is a member of the Diabetic Foot Society of India.
Why Wound Debridement Is Essential — Especially for Diabetic Patients
Every wound has a natural healing sequence: haemostasis, inflammation, proliferation, and remodelling. Necrotic tissue — whether black and dry (eschar) or yellow and soft (slough) — disrupts this sequence at every stage. It physically blocks new cell migration, triggers chronic inflammation, and creates a warm, nutrient-rich environment where bacteria multiply rapidly.
The consequences of inadequate debridement include:
- Wound infection spreading to surrounding skin, soft tissue, and bone
- Biofilm formation — a protective bacterial matrix that resists antibiotics and the immune system
- Delayed or failed healing, leading to chronic wounds that last months or years
- In diabetic patients: osteomyelitis (bone infection), gangrene, and ultimately amputation
For diabetic patients specifically, two factors make this even more critical. First, peripheral neuropathy silences the pain signals that would normally warn you a wound is deteriorating. Second, reduced peripheral circulation impairs the delivery of oxygen and immune cells that would otherwise fight infection. Together, these mean that a diabetic wound can progress from manageable to limb-threatening faster than almost any other wound type.
How Do Specialists Choose the Right Debridement Method?
There is no single ‘best’ debridement method. Selection is the result of a careful clinical assessment that weighs multiple factors. At Divyam-RDFC (Reconstructive Diabetic Foot Care), this assessment integrates:
- Wound bed composition: What percentage is necrotic tissue, slough, granulation, or epithelium? Is it dry and leathery or wet and infected?
- Infection profile: Are there signs of local or systemic infection? Has a wound swab identified specific organisms, particularly resistant strains such as MRSA?
- Vascular status: Ankle-Brachial Index (ABI) measurements and clinical vascular assessment determine whether the wound has adequate blood supply to tolerate and recover from debridement. An ischaemic limb may not be suitable for aggressive sharp debridement without prior vascular intervention.
- Plantar pressure assessment: For foot wounds, understanding where abnormal pressure is concentrated guides both debridement planning and offloading strategies.
- Patient health and tolerance: Glycaemic control, nutritional status, renal function, immune status, and the patient’s ability to attend regular appointments all influence the choice.
- Care setting: Some methods require a sterile clinical environment and specialist skill; others can be safely managed at home with proper training.
In practice, methods are frequently combined. A surgeon may perform sharp debridement to remove the bulk of necrotic tissue acutely, and then prescribe enzymatic or autolytic maintenance debridement as the wound transitions toward healing. This sequenced, multimodal approach is the standard at specialist wound care centres.
The 5 Types of Wound Debridement: A Detailed Clinical Breakdown
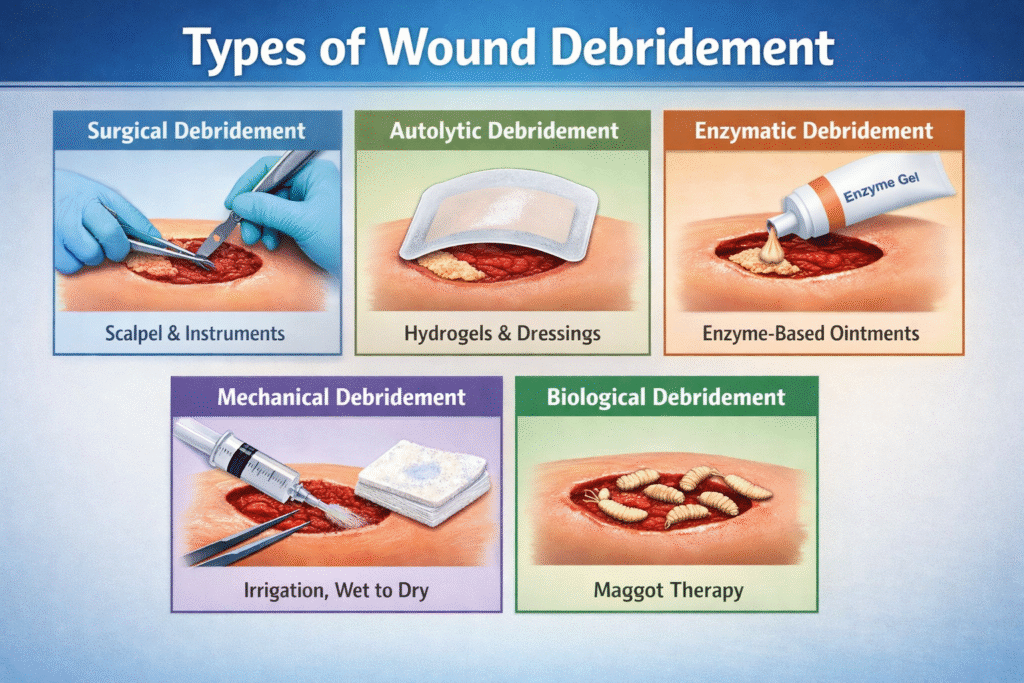
1. Surgical (Sharp) Debridement
Surgical debridement — also known as sharp debridement — is the fastest and most definitive method available. A qualified surgeon uses sterile instruments including scalpels, scissors, curettes, and rongeurs to physically excise all non-viable tissue in a controlled manner. When performed correctly, it can transform a wound obscured by necrotic eschar into a clean, bleeding wound bed within a single session.
Sharp debridement operates at two levels:
- Clinic or bedside sharp debridement: For moderate wounds, a trained wound care surgeon performs debridement under local anaesthesia in an outpatient setting. This avoids theatre costs and allows frequent, serial debridement sessions.
- Theatre-based surgical debridement: For extensive necrosis, deep wounds involving exposed bone or tendon, or patients who cannot tolerate clinic procedures, debridement is performed under regional or general anaesthesia. This also allows simultaneous procedures such as bone biopsy, wound culture, or preparation for skin grafting.
At Divyam – RDFC, surgical debridement is performed exclusively by reconstructive plastic surgeons — not general wound nurses or technicians. This distinction matters enormously. Plastic surgeons are trained to differentiate viable from non-viable tissue under direct vision, to respect critical anatomical structures such as tendons and neurovascular bundles, and to assess whether primary reconstruction (flap or graft) is needed concurrently.
Best suited for:
- Heavily infected or gangrenous wounds requiring immediate tissue removal
- Diabetic foot ulcers with bone involvement or exposed tendon
- Wounds that have failed to respond to weeks of conservative management
- Pre-operative preparation before skin grafting or flap reconstruction
Advantages:
- Immediate, complete removal of non-viable tissue in a single visit
- Allows simultaneous sampling for wound culture and histology
- Creates a clean wound bed that responds quickly to advanced dressings and grafts
Limitations:
- Requires specialist surgical expertise and equipment
- May need anaesthesia, particularly for larger or deeper wounds
- Not appropriate for ischaemic wounds without prior vascular revascularisation
2. Autolytic Debridement
Autolytic debridement is the most physiologically natural method. It works by creating a moist wound environment using specialised dressings — such as hydrogels, hydrocolloids, transparent films, or foam dressings — that trap the wound’s own moisture. Within this environment, the body’s endogenous enzymes (proteases and collagenases) and phagocytic immune cells selectively break down and digest necrotic tissue over several days to weeks.
This method is inherently selective: it digests only dead tissue and leaves healthy tissue untouched. Because it relies on the body’s own biology, it requires minimal clinical intervention — the wound is dressed and left for the dressing interval to work.
Best suited for:
- Wounds with small-to-moderate amounts of slough or soft necrosis
- Patients who are not surgical candidates due to age, comorbidities, or patient preference
- Post-debridement maintenance — to manage residual slough between surgical sessions
- Palliative or home-care settings where wound bed preparation is supportive rather than curative
Advantages:
- Painless and non-traumatic — ideal for patients with low pain tolerance
- Highly selective — no risk of removing healthy tissue
- Simple to apply and manage in community or home settings
Limitations:
- Slow — may take days to weeks to achieve meaningful debridement
- Absolutely contraindicated in clinically infected wounds — the moist environment can accelerate bacterial proliferation
- Not suitable for thick, dry eschar without first scoring or cross-hatching the surface to allow moisture penetration
Important: Never apply autolytic debridement dressings to a wound showing signs of active infection — redness spreading beyond the wound edge, increasing warmth, purulent discharge, or systemic fever. This requires prompt surgical or medical review.
3. Enzymatic (Chemical) Debridement
Enzymatic debridement involves applying a topical preparation containing exogenous proteolytic enzymes directly to the wound surface. The most widely used agent is collagenase, which selectively cleaves denatured collagen within necrotic tissue — the protein matrix that binds dead tissue to the wound bed. This loosens and liquefies the eschar or slough, allowing it to be removed during dressing changes.
The key advantage over autolysis is speed and control: enzymatic preparations actively digest necrotic tissue rather than relying purely on the body’s slower biological processes. They are typically applied once or twice daily under an appropriate secondary dressing.
Best suited for:
- Wounds with moderate necrotic burden where surgical debridement is not immediately available or indicated
- Maintaining a clean wound bed between scheduled surgical debridement sessions
- Patients in outpatient wound care programmes who attend regular clinic appointments
- Wounds transitioning from acute to subacute management
Advantages:
- More active than autolysis — begins working within hours of application
- Selective for necrotic collagen — leaves viable tissue intact
- Can be used in outpatient settings without surgical facilities
Limitations:
- Higher cost than basic wound dressings
- Certain antiseptics — notably povidone-iodine and hydrogen peroxide — deactivate collagenase and must not be used concurrently
- Requires consistent patient adherence to daily dressing changes
- Not a standalone solution for heavily infected or severely necrotic wounds
4. Mechanical Debridement
Mechanical debridement uses physical force to dislodge and remove necrotic tissue and wound debris. Several techniques fall under this category:
- Wet-to-dry dressings: Saline-moistened gauze is placed on the wound and allowed to dry, adhering to necrotic tissue. Removal strips away the dead material — but also any fragile new granulation tissue underneath.
- Wound irrigation: Pressurised saline solution is used to physically flush debris, bacteria, and loose necrotic material from the wound cavity. Pulsed lavage devices are commonly used in clinical settings.
- Hydrotherapy (whirlpool): The wound is immersed in or exposed to a stream of water to loosen and remove slough. Less commonly used in modern wound care due to infection-control concerns.
- Monofilament debridement pads: Soft abrasive fibre pads that mechanically remove surface biofilm and loose slough without causing significant tissue trauma.
Best suited for:
- Traumatic wounds with contamination, debris, or foreign bodies
- Wounds with loose, superficial slough where irrigation is sufficient
- Post-surgical irrigation of wound cavities
Advantages:
- Low cost and widely available — requires no specialist agents
- Irrigation is safe and effective for contaminated wounds
Limitations:
- Non-selective: wet-to-dry dressings remove healthy granulation tissue alongside dead tissue, causing pain and setting back healing
- Wet-to-dry dressings are no longer recommended by most advanced wound care guidelines precisely because of this non-selectivity
- Hydrotherapy carries infection-control risks in open wounds
Modern wound care has largely moved away from wet-to-dry dressings as a primary debridement strategy. If your current wound management still relies on this method and your wound is not progressing, it is worth seeking a specialist review.
5. Biological Debridement (Maggot Therapy / Larval Therapy)
Biological debridement — more commonly known as maggot therapy or larval therapy — uses sterile, laboratory-reared larvae of the Lucilia sericata (greenbottle blowfly) species. These larvae are applied to the wound in a contained dressing and left for 48–72 hours. During this time, they perform three simultaneous actions:
- Debridement: The larvae secrete powerful proteolytic enzymes that liquefy necrotic tissue, which they then ingest — leaving healthy tissue completely unharmed.
- Disinfection: Their secretions contain antimicrobial compounds that are effective against bacteria including MRSA and other antibiotic-resistant organisms that are increasingly problematic in diabetic foot infections.
- Stimulation of healing: Some research suggests that larval secretions also promote the growth of granulation tissue, though the mechanism is still being studied.
Larvae are supplied in two forms: free-range (applied directly to the wound) or contained within a mesh bag (biobag), which prevents larval migration while still allowing secretions to contact the wound surface. The biobag format is generally better tolerated by patients.
Best suited for:
- Chronic, non-healing wounds with significant slough that have not responded to other methods
- Wounds colonised with antibiotic-resistant organisms such as MRSA
- Patients who are not fit for surgical debridement
- Wounds where surgical intervention is being considered but the wound bed needs preparation first
Advantages:
- Highly selective — larvae ingest only dead tissue
- Dual action: simultaneous debridement and antimicrobial activity
- Evidence-supported for MRSA-colonised wounds
Limitations:
- Patient and caregiver acceptance can be a significant barrier
- Requires specialist availability and careful wound containment
- Not appropriate for bleeding wounds or wounds in highly vascular areas
Divyam – RDFC’s Approach: Why Specialist Assessment Transforms Wound Outcomes
There is an important distinction between wound dressing and wound care. Wound dressing is a task — applying a material to cover a wound. Wound care is a clinical discipline — assessing, diagnosing, planning, treating, and monitoring a wound through its entire healing journey. Debridement sits firmly in the second category.
At Divyam – RDFC, every patient presenting with a complex or non-healing wound undergoes a structured multi-dimensional assessment before any debridement decision is made. This includes:
- Detailed wound photography and measurement to track progress objectively
- Vascular assessment including Ankle-Brachial Index (ABI) measurement — because debridement of a severely ischaemic limb without prior revascularisation can accelerate rather than prevent amputation
- Plantar pressure assessment using pressure mapping technology to identify offloading needs that must be addressed alongside debridement for foot wounds to heal
- Microbiological assessment — wound swab or tissue biopsy to guide antibiotic selection and identify resistant organisms
- Systemic assessment — blood glucose, nutritional status, and renal function, all of which profoundly affect wound healing capacity
Dr. Sumitra Gantayet, the lead surgeon at RDFC, brings fellowship-level training in reconstructive surgery with specific expertise in diabetic foot reconstruction. She is a member of the Association of Plastic Surgeons of India, the Indian Society for Surgery of the Hand (ISSH), and the Diabetic Foot Society of India — the national body specifically focused on evidence-based diabetic limb preservation.
“Our goal is never simply to clean a wound. It is to understand why the wound exists, treat the cause, prepare the wound bed with the right debridement method, and give the body every advantage it needs to heal. Limb preservation is the outcome. Debridement is one of the most powerful tools in achieving it.”
Patients at Divyam – RDFC also benefit from post-debridement care planning: structured follow-up appointments, dressing protocols, glycaemic optimisation guidance, and — where appropriate — planning for reconstructive procedures including skin grafts, flap surgeries, or microsurgical reconstruction.
How Often Does Wound Debridement Need to Be Repeated?
Debridement is rarely a one-time event. Most chronic wounds — particularly diabetic foot ulcers — require serial debridement over the course of their healing journey. The frequency depends on the method being used, the rate at which the wound produces new necrotic tissue, and how quickly the wound bed is progressing.
As a general guide:
- Surgical sharp debridement: Typically performed every 1–4 weeks depending on wound status, with bedside sharp debridement possible at each clinic visit
- Enzymatic debridement: Daily application, usually at each dressing change
- Autolytic debridement: Dressings changed every 2–7 days depending on the product and wound condition
- Biological (larval) therapy: Applied for 48–72 hours per treatment cycle, repeated as needed
Your wound care team will set a personalised schedule and reassess at every visit. Objective measurement — wound area, depth, percentage of necrosis versus granulation — guides when to change strategy, intensify debridement, or transition to reconstruction.
When Should You Seek Urgent Wound Care?
Not all wounds need emergency attention, but certain signs require same-day or emergency review — particularly in diabetic patients. Contact your wound care team or present to emergency care immediately if you notice:
- Rapidly spreading redness, warmth, or swelling around a wound
- Foul-smelling discharge or sudden increase in wound size
- Black, blue, or dark discolouration appearing in or around the wound
- Fever, chills, or feeling systemically unwell in the context of an existing wound
- A wound that was previously stable suddenly becoming more painful — or, paradoxically, a previously painful wound that becomes completely painless (a sign of worsening neuropathy or gangrene)
Divyam – RDFC provides emergency wound care 24/7 at our Visakhapatnam clinic. Early intervention is the single most important factor in preventing limb loss.
Frequently Asked Questions About Types of Wound Debridement
Q1: Is wound debridement painful?
It depends on the method and the individual. Surgical (sharp) debridement typically requires local or general anaesthesia to ensure comfort. Autolytic and enzymatic debridement are generally painless, as they work gradually with minimal physical disruption to the wound. Mechanical methods such as wet-to-dry dressings can be painful on removal — one of the reasons they have largely been replaced by less traumatic alternatives. Your care team will discuss pain management options before any procedure.
Q2: How do I know which type of debridement my wound needs?
This decision requires a clinical assessment by a qualified wound care specialist. The type, depth, infection status, and your vascular and overall health profile all determine the right method. At RDFC, this assessment is performed by a consultant reconstructive plastic surgeon, not a general nurse or technician. If your wound has not improved after several weeks of treatment, seeking a specialist review is strongly advised.
Q3: Can wound debridement be done at home?
Some forms of maintenance debridement — particularly autolytic and enzymatic methods — can be managed at home with proper patient or caregiver training and regular clinical review. However, surgical debridement must be performed in a clinical setting by a trained specialist. Attempting sharp debridement at home is dangerous and can cause serious injury or infection. Home wound management should always be guided by and supervised by a wound care professional.
Q4: Does wound debridement help prevent amputation in diabetic patients?
Yes — in many cases, timely and appropriate debridement is one of the most effective tools for preventing amputation. By removing infected and necrotic tissue before it spreads to bone or deeper structures, debridement interrupts one of the primary pathways that leads to limb loss. However, it is most effective as part of a comprehensive care plan that includes glycaemic control, vascular assessment, offloading, infection management, and appropriate reconstruction where needed. At RDFC, limb preservation through an integrated approach is our primary clinical goal.
Q5: How long does it take for a wound to heal after debridement?
Healing timelines vary significantly depending on wound size and depth, underlying conditions such as diabetes and peripheral arterial disease, the patient’s nutritional status and blood sugar control, and whether the correct debridement method was selected and applied consistently. Superficial wounds with a clean bed may show significant progress within two to four weeks. Complex diabetic foot ulcers may require months of staged treatment, including multiple debridement sessions and potentially reconstructive procedures. Regular clinical review and objective measurement are essential to track progress and adjust the care plan accordingly.
Get Expert Wound Debridement Care at RDFC, Visakhapatnam
If you or a loved one has a wound that is not healing — particularly a diabetic foot ulcer — please do not wait and watch. Every week of delay with an untreated necrotic wound increases the risk of deep infection, osteomyelitis, and the need for major surgery. Early, expert-led debridement is the most effective way to protect your limb and your quality of life.
Why patients choose Divyam – RDFC:
- Reconstructive plastic surgeons with fellowship-level specialist training — not general practitioners
- Comprehensive pre-debridement assessment: vascular, pressure, microbiological, and metabolic evaluation
- Full range of debridement options: surgical, enzymatic, autolytic, and biological — selected based on your specific wound
- Advanced reconstructive options: skin grafts, flap surgery, and microsurgery for complex cases
- Structured post-debridement follow-up and long-term preventive care planning
- Emergency wound care available 24 hours a day, 7 days a week
Patients travel from across Andhra Pradesh, Odisha, and Telangana to access specialist wound care at RDFC. Our Visakhapatnam clinic is located at 2nd Floor, Coastal One, Plot No. 1, Balaji Nagar, Siripuram, Visakhapatnam 530003.
Book your wound care consultation today: rdfc.in/contact | Call: +91 88867 35004 (24/7 Emergency Line)