
Introduction: A Small Wound That Becomes a Big Problem
You notice something on your foot. It might be a blister from your new shoes — or it could be something far more serious.
For someone without diabetes, the answer is usually simple. For the 77 million Indians living with diabetes, that same question can mean the difference between a quick band-aid fix and a hospital admission.
Diabetic ulcers are one of the most underestimated complications of diabetes. They often start silently — a small sore, a painless patch of skin, sometimes even what looks like an ordinary blister — and they can escalate rapidly if left untreated. According to health data, up to 25% of people with diabetes will develop a foot ulcer at some point in their lives, and they are the leading cause of non-traumatic lower limb amputations worldwide.
So if you have diabetes and you spot something unusual on your foot, you need to know: Is this a diabetic ulcer or just a blister?
In this guide, we break down the key differences between diabetic ulcers and blisters, explain why diabetic foot wounds are so dangerous, walk you through the warning signs you should never ignore, and tell you exactly when to seek medical help.
What Is a Diabetic Ulcer?
A diabetic ulcer — also called a diabetic foot ulcer (DFU) — is an open sore or wound that develops on the skin of a person with diabetes, most commonly on the feet or lower legs. These ulcers form because of a combination of factors that are unique to diabetes:
Peripheral Neuropathy
High blood sugar over time damages the nerves in the feet and legs — a condition called peripheral neuropathy. When nerves are damaged, you lose the ability to feel pain, heat, and pressure. This means a small cut, blister, or pressure sore can go completely unnoticed for days or even weeks.
Poor Circulation (Peripheral Arterial Disease)
Diabetes also damages blood vessels. Poor circulation means that when a wound does form, the body struggles to deliver the oxygen, white blood cells, and nutrients needed for healing. A wound that a healthy person would heal in a week may persist for months in someone with poorly controlled diabetes.
Compromised Immune Response
High blood glucose impairs the activity of white blood cells, making it harder for the body to fight off infection. This is why a small wound in a diabetic person can become deeply infected very quickly.
Skin Changes
Diabetes often causes the skin on the feet to become dry, cracked, and thickened — especially around the heels. These cracks can become entry points for bacteria.
A diabetic ulcer typically begins at a pressure point — the ball of the foot, the heel, the tip of a toe — and may start as a red spot, a callus, or yes, even something that looks like a blister.
What Is a Blister?
A blister is a pocket of fluid — usually clear, watery serum — that forms between the upper layers of the skin. They are the body’s way of protecting damaged tissue underneath.
Blisters form due to:
- Friction — ill-fitting shoes rubbing against the skin
- Burns — heat, sunburn, or chemical exposure
- Allergic reactions — to materials, soaps, or chemicals
- Infections — such as chickenpox or herpes zoster (shingles)
- Autoimmune conditions — like bullous pemphigoid
For most people, a blister is a minor inconvenience. The fluid inside cushions the tissue, the blister eventually reabsorbs or pops, and the skin heals on its own within a week or two.
But for people with diabetes, even an ordinary friction blister can quickly become dangerous.
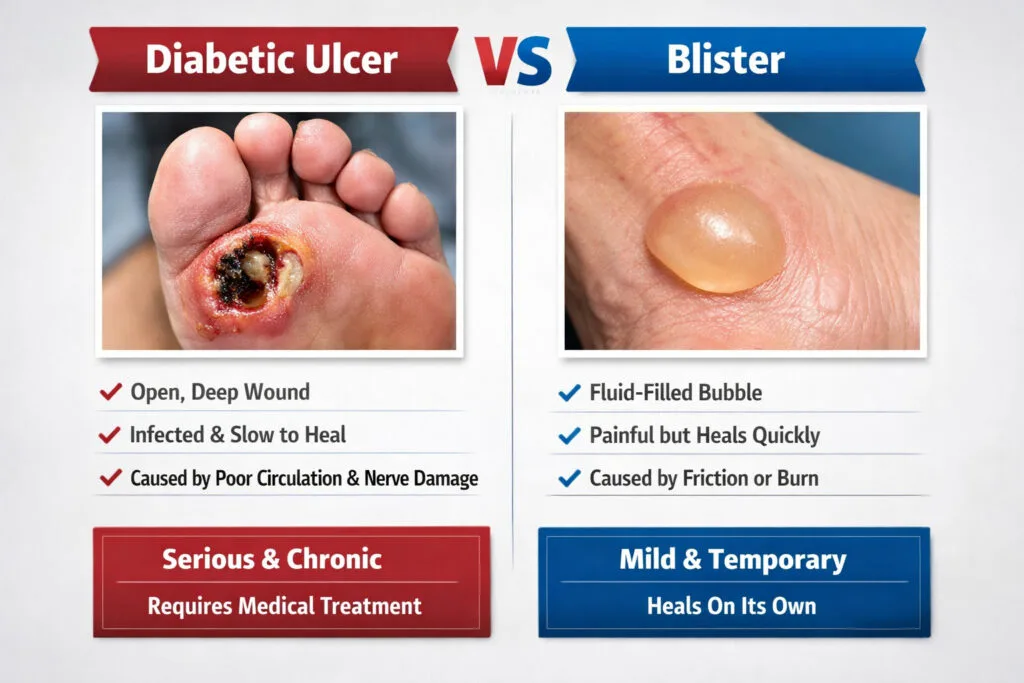
Diabetic Ulcer vs Blister: Key Differences at a Glance
| Feature | Diabetic Ulcer | Ordinary Blister |
|---|---|---|
| Cause | Neuropathy, pressure, poor circulation | Friction, burn, allergy, infection |
| Fluid inside | May be absent; often open/dry | Usually clear fluid (serum) |
| Pain | Often painless (due to neuropathy) | Usually painful or tender |
| Appearance | Red, dark, crusty, or open wound; may have black edges | Raised fluid-filled bubble, intact skin |
| Location | Ball of foot, heel, tips of toes, pressure points | Anywhere; common on heels, toes |
| Healing speed | Very slow or does not heal | Usually heals in 1–2 weeks |
| Risk of infection | Very high | Low in healthy individuals |
| Surrounding skin | May be thickened (callus), discoloured, warm or cool | Usually normal |
| Odour | May be present if infected | Absent |
| Depth | Can be superficial or extend to tendon/bone | Superficial only |
How to Tell If It’s a Diabetic Ulcer: 7 Warning Signs
If you have diabetes and you notice a wound on your foot, look for these signs that it may be more than just a blister:
1. You Don’t Feel Pain — But You Should
A normal blister hurts when you press it. If you have a wound and you feel no pain at all — or very little — this is a red flag. It likely means peripheral neuropathy has dulled your sensation. This is actually more dangerous than a painful wound, because pain-free wounds tend to go unnoticed and worsen.
2. The Wound Isn’t Healing After Two Weeks
Healthy blisters typically heal within one to two weeks. If your wound has been present for more than two weeks without significant improvement, it is likely a chronic wound — a hallmark of diabetic ulcers. Do not wait any longer; seek medical care immediately.
3. The Edges Look Dark or Black
A diabetic ulcer that has developed poor blood supply may show blackening or darkening around the edges. This can indicate gangrene — tissue death — which is a medical emergency.
4. There Is Redness, Swelling, or Warmth Spreading Around the Wound
These are signs of infection. If the redness is spreading outward from the wound, the area is swollen, and the skin feels warm to the touch, bacteria have likely spread into the surrounding tissue — a condition called cellulitis.
5. There Is an Unpleasant Odour
Infected wounds produce a distinctive smell due to bacterial activity. Any foul odour from a foot wound in a diabetic person needs immediate medical attention.
6. The Wound Is Draining Yellow, Green, or Brown Fluid
Clear fluid is normal in a blister. But if the fluid inside or around your wound is yellow, green, or brown — especially if it is thick — this signals bacterial infection.
7. You Can See Yellow Tissue, Tendons, or Bone
This may sound alarming — because it is. Diabetic ulcers can be deceptively deep. What looks like a small surface wound can extend all the way to the bone. If you can see any yellow, white, or dark tissue at the base of the wound, see a specialist immediately. This indicates a full-thickness wound requiring urgent care.
Diabetic Blisters (Bullosis Diabeticorum): A Special Case
There is one more important condition to know about: bullosis diabeticorum, or diabetic blisters.
These are spontaneous blisters that appear in people with diabetes — usually on the feet, lower legs, hands, or forearms — with no apparent cause. They are not caused by friction or injury. They simply appear, often overnight.
Diabetic blisters tend to be:
- Large (sometimes several centimetres across)
- Filled with clear, sterile fluid
- Painless
- Located on the top of the feet or toes, or on the lower legs
Although they are not ulcers themselves, they carry serious risks in diabetic patients:
- If they rupture, the open wound becomes a portal for infection
- Poor healing ability means they can deteriorate into a true ulcer
- Their painlessness means they may go unnoticed until they break open
Never attempt to pop or drain a diabetic blister at home. Always consult a wound care specialist.
Why Diabetic Foot Wounds Are So Dangerous: The Cascade Effect
Understanding why diabetic ulcers are so serious requires understanding the cascade of complications that can follow a simple untreated wound:
Day 1–3: A small blister or pressure sore develops. Because of neuropathy, you don’t feel it.
Day 4–10: The wound remains open, bacteria begin colonising the wound. Blood sugar levels rise due to infection, which further impairs healing and immune response.
Week 2–4: Infection spreads deeper into the tissue (deep tissue infection). Redness and swelling spread. If the bone is nearby, bacteria can infect it — causing osteomyelitis.
Week 4+: Without treatment, gangrene can set in. At this point, amputation of the toe, foot, or even the leg may become necessary to save the person’s life.
This entire cascade can begin with something as simple as a friction blister or a small cut — and it can happen faster than most people expect.
How to Check Your Feet If You Have Diabetes
The best way to prevent a small wound from becoming a diabetic ulcer is a daily foot inspection. Here’s how to do it properly:
Step-by-Step Daily Foot Check
Choose a consistent time — after a bath or shower is ideal, when the skin is clean.
Use good lighting — sit near a window or use a bright lamp.
Use a mirror or ask for help — checking the soles of your feet is difficult without assistance. A handheld mirror or a mirror on the floor can help you see the undersides.
Check every surface — tops of toes, between toes, balls of feet, arches, heels, and ankles.
Look for:
- Any new redness, swelling, or discolouration
- Cuts, cracks, blisters, or fluid-filled bumps
- Dry or peeling skin
- Thickened or discoloured toenails
- Any changes in skin temperature (one foot warmer or cooler than the other)
- Any wound that was there yesterday but seems larger today
Record what you find — a simple photo on your phone dated each day can help you and your doctor track changes.
If you find anything unusual, do not wait to see if it gets better on its own. Contact your diabetes care team or a wound care specialist the same day.
What to Do If You Find a Foot Wound
Here is a simple action plan for anyone with diabetes who discovers a foot wound:
If the Wound Is a Small, Intact Blister With No Redness or Swelling:
- Clean the area gently with mild soap and water
- Apply a clean, non-stick dressing to protect it
- Do NOT pop or drain the blister
- Reduce pressure on the area — avoid tight shoes, rest the foot
- Monitor twice daily for any changes
- Call your doctor or wound care specialist the same day to report it
If the Wound Is Open, Draining, Painful, or Looks Like an Ulcer:
- Do not attempt to treat it at home
- Do not apply home remedies, turmeric paste, or any substance not prescribed by a doctor
- Clean it gently and cover with a clean bandage
- Go to a wound care clinic or emergency department immediately
- Bring a list of your current medications and recent blood sugar readings
If There Is Blackening, Severe Swelling, or Fever:
- This is a medical emergency
- Go to the nearest hospital emergency department immediately
- Do not delay
Treatment for Diabetic Ulcers — What to Expect
If you are diagnosed with a diabetic ulcer, treatment will depend on the severity of the wound. A wound care specialist will classify the ulcer using a grading system (such as the Wagner or University of Texas scale) and recommend a treatment plan.
Wound Debridement
Dead or infected tissue must be removed to allow healthy tissue to grow. This is called debridement and is done by a trained clinician — never attempt to remove dead tissue at home.
Offloading
Reducing pressure on the wound is critical. This may involve special footwear, total contact casting, or crutches to keep weight off the affected area.
Wound Dressings
Modern wound dressings do far more than simply cover a wound. Depending on the type and stage of your ulcer, your doctor may use:
- Antimicrobial dressings (for infected wounds)
- Moisture-retaining dressings (to support tissue regrowth)
- Negative pressure wound therapy (vacuum-assisted closure)
- Bioengineered skin substitutes
Blood Sugar Control
This is non-negotiable. Even the best wound care will fail if blood glucose levels remain uncontrolled. Your care team will work with your diabetologist or endocrinologist to optimise your diabetes management during healing.
Antibiotics
If the wound is infected, oral or intravenous antibiotics will be prescribed based on culture results. Always complete the full course.
Vascular Intervention
If poor circulation is contributing to the ulcer, a vascular surgeon may recommend procedures to improve blood flow — such as angioplasty or bypass surgery.
Preventing Diabetic Ulcers — Practical Steps You Can Take Today
Prevention is always better than treatment. Here are evidence-based steps to protect your feet:
Control your blood sugar — this is the single most important thing you can do. Consistently high glucose damages nerves and blood vessels, the two key drivers of ulcer risk.
Never walk barefoot — even at home. Always wear properly fitted, cushioned footwear that protects your feet from cuts, burns, and pressure.
Choose footwear carefully — shoes should fit comfortably without rubbing. Many people with diabetes benefit from custom orthotic footwear. Have your feet measured every time you buy shoes; foot shape can change.
Inspect your shoes before wearing them — run your hand inside your shoes each time before putting them on. A small stone, seam, or folded insole can cause a wound you won’t feel.
Keep your feet moisturised — apply a good foot cream daily to prevent dry, cracked skin. Avoid applying cream between the toes, as this can encourage fungal infections.
Trim toenails carefully — cut straight across, not into the corners. If you have reduced sensation or poor vision, have a podiatrist trim your nails.
Stop smoking — smoking severely impairs blood circulation and dramatically increases the risk of diabetic foot complications.
See a podiatrist regularly — a foot specialist can identify and treat calluses, nail problems, and early pressure sores before they become ulcers.
Attend your diabetes check-ups — annual foot examinations should be part of every diabetic person’s care plan. Do not skip them.
FAQ: Diabetic Ulcer vs Blister
1. Can a blister turn into a diabetic ulcer?
Yes, absolutely. This is one of the most common ways diabetic ulcers develop. A friction blister or minor wound that would heal normally in someone without diabetes can quickly become an infected, non-healing wound — a true ulcer — in someone with diabetes. This is why any foot wound in a diabetic person must be taken seriously from day one.
2. How do I know if my foot wound is infected?
Signs of infection include increasing redness, warmth, and swelling around the wound; yellow, green, or brown discharge; a foul smell; red streaks spreading from the wound; and fever or chills. Any of these symptoms require immediate medical attention.
3. Is it safe to pop a blister if I have diabetes?
No. Popping a blister — even with a needle — creates an open wound that is highly vulnerable to infection. In a person with diabetes, that infection can spread rapidly. Always consult a healthcare provider before doing anything to a blister on your feet.
4. Do diabetic ulcers always hurt?
Not always — and this is what makes them especially dangerous. Many diabetic ulcers are painless because peripheral neuropathy has damaged the nerve endings in the foot. A painless ulcer can become deeply infected before the person even realises something is wrong. This is why daily foot inspections are so important.
5. When should I go to hospital for a foot wound?
Go immediately if you notice: a wound that is blackening around the edges; spreading redness, severe swelling, or red streaks; fever or chills accompanying a foot wound; a foul smell; or if you can see tissue or bone at the base of the wound. These are all signs of a serious infection or gangrene that requires emergency care.
When to See a Specialist at RDFC
At Divyam – RDFC (rdfc.in), our wound care specialists are experienced in diagnosing and treating diabetic foot wounds at every stage — from early blisters to complex ulcers requiring advanced wound management.
You should schedule an appointment with us if you:
- Have diabetes and notice any new wound, blister, or skin change on your feet or lower legs
- Have a wound that has not healed after two weeks
- Have been told you have peripheral neuropathy or poor circulation
- Have a history of previous diabetic ulcers or foot infections
- Want a comprehensive diabetic foot assessment to protect your long-term health
Don’t wait for a small wound to become a big problem. Early intervention is the most effective — and often the least invasive — form of treatment.
👉 Book your wound care consultation at RDFC today — rdfc.in
Conclusion: Know the Difference, Protect Your Feet
The difference between a diabetic ulcer and a blister might seem subtle — but the consequences of getting it wrong can be life-changing.
A blister in a healthy person is a minor inconvenience. In someone with diabetes, that same blister can be the first step in a cascade that leads to infection, hospitalisation, and — in the worst cases — amputation.
The good news is that diabetic foot complications are largely preventable with the right knowledge, daily vigilance, and timely professional care. By learning to recognise the warning signs of a diabetic ulcer versus a harmless blister, and by acting quickly when something doesn’t look right, you can protect your feet, your mobility, and your quality of life.
If you are living with diabetes, make foot care a non-negotiable part of your daily routine. And if you ever have any doubt about a wound on your feet — no matter how small it seems — speak to a specialist.
Your feet carry you through life. Take care of them.
For expert wound care and diabetic foot management, visit RDFC — rdfc.in.