
Wagner’s classification of diabetic foot is the most widely used grading system to assess the severity of diabetic foot ulcers and wounds. It helps doctors determine the right treatment, predict outcomes, and prevent amputation. In this guide, we break down every grade in plain language — so you know exactly what you’re dealing with and what to do next.
What Is Wagner’s Classification of Diabetic Foot?
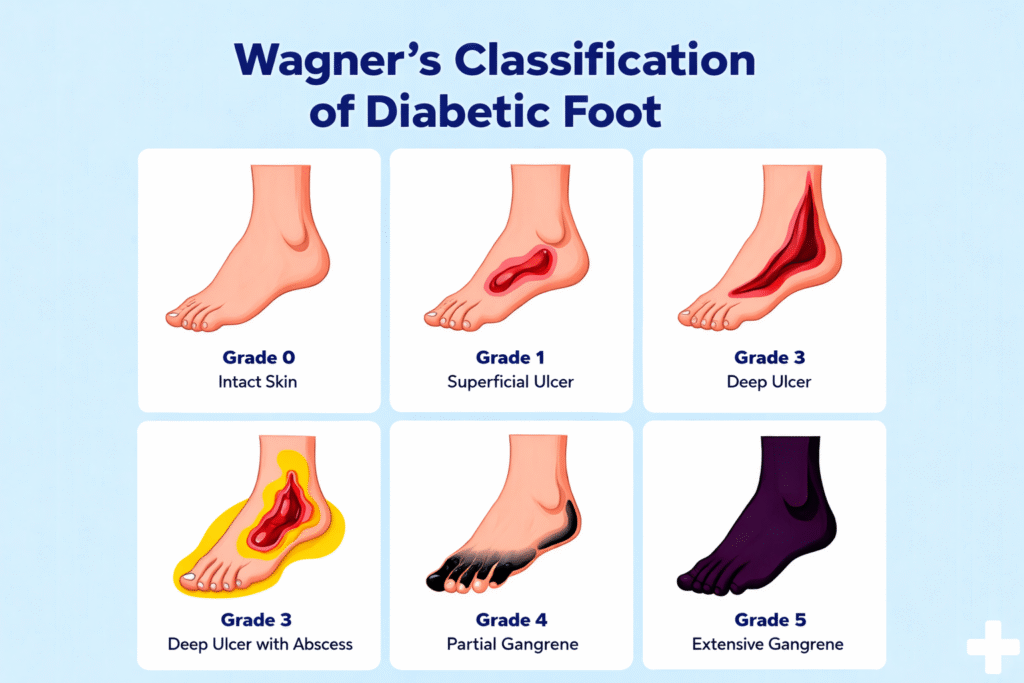
Wagner’s classification, is a six-grade (Grade 0 to Grade 5) system used to evaluate diabetic foot wounds based on depth, infection, and involvement of deeper structures like bone or joints.
It remains the gold standard in clinical practice because it is simple, practical, and directly guides treatment decisions. Whether you’re a patient, caregiver, or healthcare professional, understanding these grades helps you communicate better with your medical team and take faster action.
Why Is Grading Diabetic Foot Wounds Important?
Diabetes damages nerves (neuropathy) and blood vessels (vasculopathy), making foot wounds slow to heal and highly prone to infection. Without grading:
- Mild wounds can be over-treated unnecessarily
- Severe wounds can be under-treated, leading to gangrene or amputation
- Treatment plans cannot be standardized across healthcare settings
Wagner’s classification solves this by giving every wound a clear, actionable score.
The 6 Grades of Wagner’s Classification — Explained Simply
Grade 0: Pre-Ulcerative Lesion (High-Risk Foot)
What it looks like: No open wound, but the foot shows warning signs — calluses, bony deformities (like bunions or hammertoes), dry cracked skin, or reduced sensation due to neuropathy.
What it means: The foot hasn’t broken down yet, but it’s at serious risk of developing an ulcer.
Treatment approach:
- Regular foot inspections (daily self-checks)
- Protective footwear and offloading insoles
- Callus debridement by a podiatrist or foot specialist
- Blood sugar control
- Patient education on foot hygiene
Key message: Grade 0 is the best time to intervene. Prevention at this stage can stop an ulcer from ever forming.
Grade 1: Superficial Ulcer (No Infection)
What it looks like: A shallow, open sore on the skin’s surface. It does not penetrate deeper tissues. No signs of infection such as redness spreading beyond the wound edge, warmth, or pus.
What it means: The protective skin barrier has broken down. This is typically caused by repeated pressure on a callus or injury that went unnoticed due to numbness.
Treatment approach:
- Wound debridement (removal of dead tissue)
- Offloading — removing pressure from the wound using special footwear, casts, or crutches
- Moist wound dressings to promote healing
- Blood glucose optimization
- Regular follow-up every 1–2 weeks
Key message: Grade 1 wounds heal well with proper care. Offloading is the single most important intervention at this stage.
Grade 2: Deep Ulcer (No Abscess, No Bone Involvement)
What it looks like: The ulcer penetrates through skin into deeper soft tissues — tendons, joint capsule, or fascia — but bone is not yet involved and there is no abscess (pocket of pus).
What it means: The wound is now entering dangerous territory. Without prompt treatment, infection can spread rapidly to bone.
Treatment approach:
- Hospital evaluation is often recommended
- Surgical debridement to clean the wound
- Swab cultures to identify bacteria and guide antibiotic therapy
- Offloading continues to be critical
- Advanced wound dressings (negative pressure wound therapy may be used)
- Vascular assessment to check blood supply to the foot
Key message: Grade 2 requires urgent specialist attention. Do not wait for it to “get better on its own.”
Grade 3: Deep Ulcer with Abscess, Osteomyelitis, or Septic Arthritis
What it looks like: A deep wound with one or more of: a pocket of infection (abscess), bone infection (osteomyelitis), or infected joint (septic arthritis). Probing the wound with a sterile instrument often reaches bone.
What it means: This is a limb-threatening condition. Bone infection (osteomyelitis) is particularly serious because bacteria embed in bone tissue and are very difficult to eradicate with antibiotics alone.
Treatment approach:
- Urgent hospitalization
- IV (intravenous) antibiotics — often for 4–6 weeks
- Surgical debridement, drainage of abscess
- Possible bone resection (removal of infected bone)
- Vascular surgery if blood flow is compromised
- MRI imaging to assess extent of bone involvement
- Multidisciplinary team: surgeon, diabetologist, vascular surgeon, microbiologist
Key message: Grade 3 is a medical emergency. Delay at this stage significantly increases amputation risk.
Grade 4: Gangrene of Part of the Foot (Forefoot or Heel)
What it looks like: Localized gangrene — tissue death — affecting a specific part of the foot, typically the toes, forefoot, or heel. The affected area appears black, dark brown, or dark purple.
What it means: Blood supply to that part of the foot has been severely compromised. The tissue is dead and cannot be saved. However, the rest of the foot may still be salvageable.
Types of gangrene:
- Dry gangrene: No infection, caused purely by poor blood supply. The tissue dries and shrivels.
- Wet gangrene: Infected, with pus, foul smell, and rapidly spreading bacteria. This is a surgical emergency.
Treatment approach:
- Emergency hospitalization
- Vascular assessment and possible revascularization (restoring blood flow via angioplasty or bypass surgery)
- Surgical debridement and amputation of dead tissue (toe or forefoot amputation)
- IV antibiotics (especially in wet gangrene)
- Reconstructive procedures post-amputation to preserve function
- Wound closure with skin grafts or flaps if needed
Key message: Amputation at Grade 4 does not mean losing the whole foot. Skilled reconstructive surgeons can often perform partial amputations that preserve walking ability.
Grade 5: Gangrene of the Whole Foot
What it looks like: Extensive gangrene involving the entire foot. The damage is so widespread that no part of the foot can be saved.
What it means: This is the most severe stage of diabetic foot disease. It carries high risk of life-threatening systemic infection.
Treatment approach:
- Emergency below-knee or above-knee amputation to save the patient’s life
- Intensive care management for sepsis
- Post-amputation rehabilitation and prosthetic fitting
- Long-term diabetes management to prevent complications in the remaining limb
Key message: Grade 5 is largely preventable. It almost always results from delayed treatment at earlier grades. Early action at Grade 1, 2, or 3 can prevent this outcome.
Wagner’s Classification at a Glance
| Grade | Description | Depth | Infection | Urgency |
|---|---|---|---|---|
| 0 | Pre-ulcerative / High-risk | Skin intact | None | Preventive care |
| 1 | Superficial ulcer | Skin only | None | Outpatient |
| 2 | Deep ulcer | Tendons/fascia | Possible | Urgent referral |
| 3 | Deep ulcer + abscess/bone | Bone/joint | Yes | Hospitalization |
| 4 | Partial foot gangrene | Full thickness | Possible | Emergency |
| 5 | Whole foot gangrene | Entire foot | Yes | Emergency surgery |
Limitations of Wagner’s Classification
While Wagner’s system is widely used, it has a few limitations worth knowing:
- Does not assess ischemia (blood supply) independently. A wound with poor blood supply heals much slower — but Wagner grades it the same as one with good circulation.
- Does not capture wound size or area.
- Does not account for neuropathy severity.
Because of these gaps, the University of Texas (UT) Wound Classification System is sometimes used alongside Wagner’s to provide a more complete picture by grading both depth and ischemia separately.
Your specialist may use both systems together to plan your care.
How Is a Diabetic Foot Wound Assessed in Clinic?
A thorough diabetic foot assessment includes more than just grading the wound. At a specialist clinic like Divyam -Reconstructive Diabetic Foot Care (RDFC), evaluation typically includes:
1. Full wound assessment
- Size, depth, and location of the ulcer
- Presence of slough, necrosis, or healthy granulation tissue
- Signs of infection (redness, warmth, odor, discharge)
2. Neurological assessment
- Monofilament testing to detect loss of protective sensation
- Vibration perception threshold
3. Vascular assessment
- Ankle-Brachial Index (ABI) to measure blood flow
- Doppler studies
- Referral for angiography if revascularization is needed
4. Imaging
- X-ray to detect gas in tissues or bony changes
- MRI for detailed assessment of osteomyelitis or abscess
5. Microbiological assessment
- Deep tissue cultures (not surface swabs) to identify causative bacteria and guide targeted antibiotic therapy
Wagner Grade and Treatment Pathway: What to Expect
Grades 0–1: Community and Outpatient Care
Most Grade 0 and 1 cases can be managed in a specialist outpatient clinic. The focus is on wound care, offloading, and preventing progression. Healing typically takes 4–12 weeks with good compliance.
Grades 2–3: Specialist Referral and Possible Hospitalization
Grade 2 and 3 wounds need prompt specialist review. Hospitalization is often required for Grade 3 to administer IV antibiotics and plan surgery. A multidisciplinary team approach gives the best outcomes.
Grades 4–5: Surgical Emergency
Grades 4 and 5 are surgical emergencies. Speed matters. The sooner vascular and surgical teams assess the patient, the higher the chance of saving the limb — or the patient’s life.
Can Diabetic Foot Ulcers Be Prevented?
Yes — and prevention is far easier than treatment. Most diabetic foot ulcers are preventable with consistent daily care:
Daily habits that protect your feet:
- Inspect your feet every day, including between the toes
- Wash feet in lukewarm water and dry thoroughly
- Moisturize daily (but not between the toes)
- Never walk barefoot — even indoors
- Wear well-fitting diabetic footwear
- Trim toenails straight across
- See a foot specialist regularly — at least once a year if you have diabetes
Medical management:
- Keep HbA1c levels in your target range
- Control blood pressure and cholesterol
- Stop smoking — it severely impairs circulation
- Attend regular vascular and podiatric check-ups
When Should You See a Diabetic Foot Specialist?
See a specialist immediately if you notice:
- Any open wound or sore on your foot, no matter how small
- Redness, warmth, or swelling around a wound
- Pus or foul smell from a wound
- Black or dark discoloration of skin or toes
- Foot pain that wakes you at night (sign of ischemia)
- Fever with a foot wound — this is an emergency
Do not wait to “see if it heals.” Diabetic foot wounds can worsen in 24–48 hours.
Conclusion: Early Grading Saves Limbs and Lives
Wagner’s classification of diabetic foot is more than a medical scoring system — it’s a roadmap for action. The earlier a wound is identified and graded, the more treatment options are available, and the better the outcome.
If you or a loved one has diabetes, don’t wait for a wound to become severe before seeking care. A specialist assessment at Grade 0 or 1 is simple, fast, and could prevent amputation down the line.
FAQ
1. What is the most dangerous grade in Wagner’s classification?
Grade 5 is the most severe, involving complete gangrene of the foot and often requiring amputation. However, Grade 3 is often the most critical turning point — bone infection at this stage can be very difficult to treat and often leads to partial amputation if not managed urgently.
2. Can a Grade 3 or 4 diabetic foot be saved without amputation?
In some cases, yes. With early specialist intervention, good blood supply, effective antibiotic therapy, and advanced reconstructive surgery, partial foot salvage is possible even at Grade 3 or 4. A specialist in reconstructive diabetic foot care will assess each case individually.
3. How long does a diabetic foot ulcer take to heal?
This depends on the grade, blood supply, blood sugar control, and treatment compliance. Grade 1 ulcers may heal in 4–8 weeks. Deeper wounds (Grade 2–3) may take 3–6 months or longer. Wounds with poor blood supply heal much more slowly.
4. Is Wagner’s classification still used today?
Yes, widely. It remains the most practical grading tool in clinical settings. It is sometimes used alongside the University of Texas system for a more complete assessment, especially in research and academic centers.
5. What is the difference between dry and wet gangrene in diabetic foot?
Dry gangrene is caused by poor blood flow alone, resulting in dry, shriveled, blackened tissue. Wet gangrene involves active bacterial infection on top of poor blood supply, with pus, foul odor, and rapid spread. Wet gangrene is a surgical emergency requiring immediate intervention.
Get Expert Diabetic Foot Care in Visakhapatnam
At Divyam-Reconstructive Diabetic Foot Care (RDFC), our team of highly qualified plastic surgeons — led by Dr. Sumitra Gantayet — specializes exclusively in diabetic foot care. We offer:
- Comprehensive wound assessment and Wagner grading
- Advanced wound care and offloading
- Vascular assessment including ABI measurements
- Reconstructive surgery: skin grafts, flaps, and microsurgery
- Offloading surgeries to reduce pressure and prevent re-ulceration
- Lifelong post-operative care and prevention education
📍 Vizag Clinic: 2nd Floor, Coastal One, Plot No. 1, Balaji Nagar, Siripuram, Visakhapatnam – 530003 📞 Call us 24/7: +91 88867 35004 🌐 Visit: https://rdfc.in/contact/