
Introduction
A diabetic foot ulcer (DFU) is not just a simple wound—it’s a complex, chronic complication of diabetes that reflects deep underlying physiological dysfunction. Imagine a small crack in a wall that slowly spreads because the foundation is weak—that’s exactly how DFUs behave. These ulcers typically occur on pressure points like the heel or the ball of the foot, and they often go unnoticed until they become severe.
What makes DFUs particularly dangerous is their silent progression. Due to nerve damage, many patients don’t feel pain, allowing minor injuries to evolve into serious wounds. Clinically, DFUs are one of the most significant causes of hospital admissions among diabetic patients. They are also the leading cause of non-traumatic lower limb amputations worldwide, making them a critical public health concern.
Beyond physical damage, DFUs drastically reduce quality of life. Patients often face prolonged hospital stays, repeated surgeries, and psychological stress. Understanding their pathophysiology is essential because prevention and treatment depend heavily on addressing the root causes rather than just treating the surface wound.
Global Burden and Prevalence
Let’s talk numbers—because they reveal just how serious this condition is. Globally, around 18.6 million people develop diabetic foot ulcers every year, and up to one-third of diabetic patients will experience a foot ulcer in their lifetime.
That’s not all. Studies show that approximately 15–25% of people with diabetes will develop DFUs at some point, and over 85% of diabetes-related amputations are preceded by foot ulcers.
Even more alarming is the recurrence rate—about 42% within one year and 65% within five years. This means even if a wound heals, the underlying issues remain, setting the stage for future complications.
Overview of Pathophysiology
Multifactorial Nature of DFU
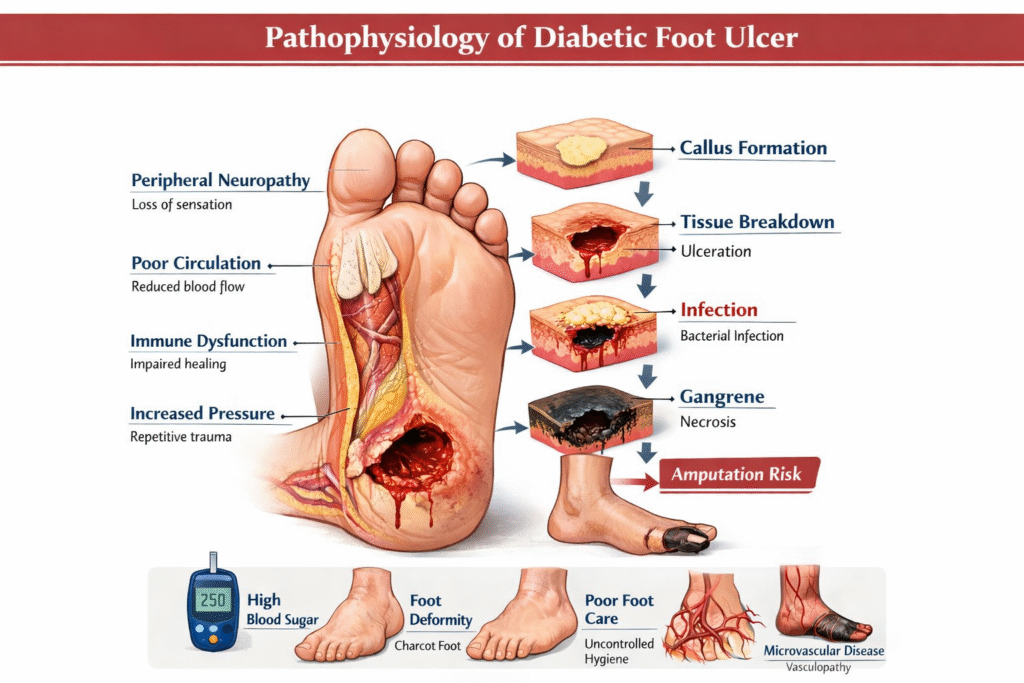
The pathophysiology of diabetic foot ulcers is like a perfect storm where multiple damaging processes converge. It’s not just one cause—it’s a combination of neuropathy, ischemia, immune dysfunction, and mechanical stress all acting together.
Think of it as a three-legged stool: remove one leg, and the stool collapses. Similarly, DFUs develop when key protective mechanisms of the body fail simultaneously. According to clinical research, the core contributors include:
- Peripheral neuropathy
- Peripheral arterial disease (PAD)
- Impaired wound healing
- Infection
Each of these factors alone can cause damage, but together, they create a highly vulnerable environment where even minor trauma can lead to ulcer formation.
Key Components Involved
At the cellular and tissue levels, the disease process involves:
- Nerve damage → Loss of sensation
- Vascular compromise → Reduced blood flow
- Immune dysfunction → Poor infection control
- Mechanical stress → Tissue breakdown
This combination results in a situation where the body cannot detect injury, cannot repair it effectively, and cannot fight infection properly.
Role of Hyperglycemia in Tissue Damage
Metabolic Changes
Chronic hyperglycemia is the starting point of all complications in diabetes, including DFUs. Elevated blood glucose levels trigger a cascade of metabolic disturbances that damage nerves, blood vessels, and tissues.
One key mechanism is the formation of advanced glycation end products (AGEs). These molecules accumulate in tissues and interfere with normal cellular function. They stiffen blood vessels, reduce elasticity, and impair oxygen delivery to tissues.
Additionally, hyperglycemia activates the polyol pathway, leading to sorbitol accumulation inside cells. This causes osmotic stress and cellular damage, particularly in nerve cells. Over time, these changes compromise the structural integrity of tissues, making them more susceptible to injury.
Oxidative Stress and Cellular Injury
Another major player is oxidative stress. High glucose levels increase the production of free radicals, which damage DNA, proteins, and cell membranes.
This oxidative damage disrupts:
- Endothelial function (affecting blood vessels)
- Immune responses
- Cellular repair mechanisms
Peripheral Neuropathy in DFU
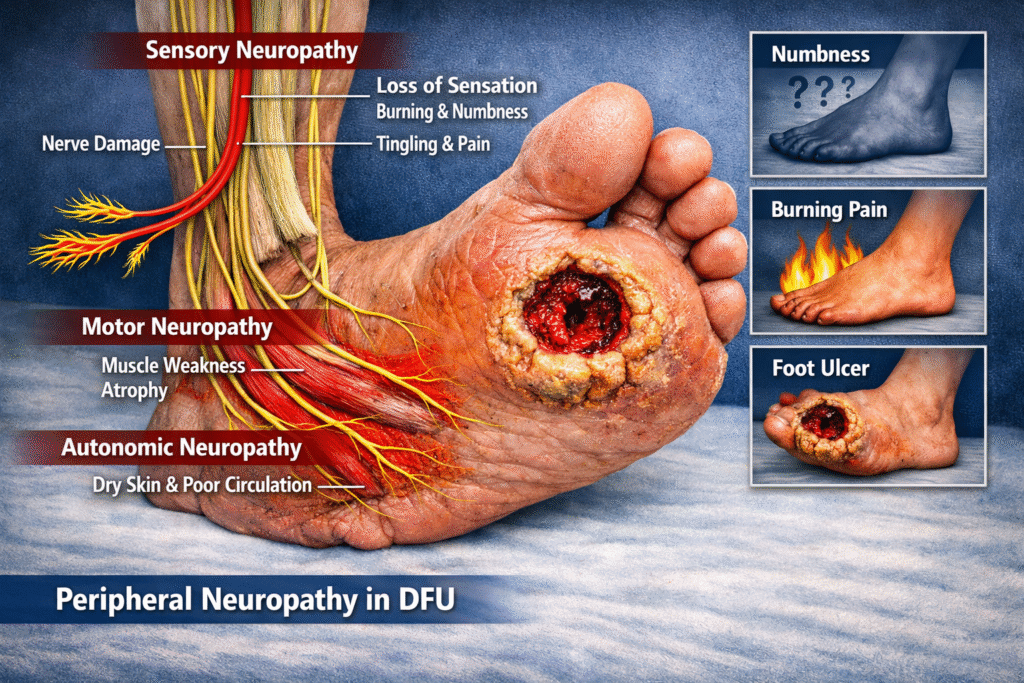
Sensory Neuropathy
Sensory neuropathy is perhaps the most critical factor in DFU development. It leads to loss of protective sensation, meaning patients cannot feel pain, heat, or pressure.
Imagine stepping on a sharp object and not realizing it—that’s the reality for many diabetic patients. Minor injuries go unnoticed and untreated, allowing them to worsen over time.
Studies show that neuropathy contributes to 60–70% of diabetic foot ulcers.
Motor Neuropathy
Motor neuropathy affects the muscles of the foot, leading to deformities such as:
- Claw toes
- Hammer toes
- Prominent metatarsal heads
These deformities alter weight distribution, creating high-pressure points that are prone to ulceration.
Autonomic Neuropathy
Autonomic neuropathy reduces sweat production, leading to dry and cracked skin. These cracks act as entry points for bacteria, increasing the risk of infection.
It also disrupts blood flow regulation, further compromising tissue health. Together, these changes create a perfect environment for ulcer formation.
Peripheral Arterial Disease
Macrovascular Changes
Peripheral arterial disease reduces blood flow to the lower limbs due to narrowing of large arteries. This leads to ischemia, where tissues do not receive enough oxygen and nutrients.
Ischemic tissues are fragile and heal poorly. Even minor injuries can progress into severe ulcers because the body lacks the resources to repair them.
Microvascular Dysfunction
In addition to large vessel disease, diabetes affects small blood vessels (microangiopathy). This further impairs oxygen delivery and waste removal at the cellular level.
The result? Delayed healing, tissue necrosis, and increased susceptibility to infection.
Biomechanical Abnormalities
Foot Deformities
Due to motor neuropathy, the architecture of the foot changes. These deformities increase pressure on specific areas, especially during walking.
Pressure Redistribution
Normally, the foot distributes weight evenly. In diabetic patients, this balance is disrupted, leading to localized pressure points.
Repeated pressure causes:
- Skin breakdown
- Callus formation
- Ulcer development
It’s like constantly rubbing the same spot until it eventually breaks open.
Impaired Wound Healing
Inflammatory Dysfunction
In diabetic patients, the inflammatory response is abnormal. Instead of progressing through normal healing stages, wounds remain stuck in a chronic inflammatory state.
Reduced Growth Factors
Growth factors like VEGF and PDGF are essential for tissue repair. In diabetes, their production is reduced, slowing down healing significantly.
As a result, wounds that would normally heal in days or weeks can persist for months.
Infection and Immune Dysfunction
Bacterial Colonization
Once the skin barrier is broken, bacteria can easily invade. DFUs are often polymicrobial, meaning multiple types of bacteria are involved.
Impaired Immunity in Diabetes
Diabetes weakens the immune system, reducing the body’s ability to fight infections. This leads to:
- Rapid spread of infection
- Tissue destruction
- Increased risk of gangrene
Approximately 50% of diabetic foot ulcers become infected, highlighting the severity of this issue.
Role of Callus Formation and Trauma
Repetitive Stress Injuries
Calluses form as a protective response to pressure, but in diabetic patients, they can become problematic. Beneath the callus, micro-hemorrhages can occur, eventually leading to ulcer formation.
Repeated trauma—whether from walking, tight shoes, or minor injuries—acts as the final trigger in the development of DFUs.
Classification Based on Pathophysiology
Neuropathic Ulcers
- Painless
- Located on pressure points
- Surrounded by callus
Ischemic Ulcers
- Painful
- Located on toes or foot edges
- Associated with poor blood flow
Neuro-Ischemic Ulcers
- Combination of both
- Most severe type
- Common in long-standing diabetes
Clinical Implications of Pathophysiology
Risk of Amputation
The ultimate consequence of DFUs is amputation. Around 20% of patients with DFUs require lower limb amputation, and the mortality rate after amputation is extremely high.
Understanding the pathophysiology helps clinicians target treatment strategies such as:
- Offloading pressure
- Improving blood flow
- Controlling infection
- Enhancing wound healing
Conclusion
The pathophysiology of diabetic foot ulcers is a complex interplay of metabolic, neurological, vascular, and immunological factors. It begins with hyperglycemia and progresses through nerve damage, poor circulation, impaired healing, and infection. Each component amplifies the others, creating a vicious cycle that leads to chronic wounds and severe complications.
Breaking this cycle requires a comprehensive approach that addresses all underlying mechanisms rather than just treating the ulcer itself. Early detection, proper foot care, and strict glycemic control remain the cornerstones of prevention.
FAQs
1. What is the main cause of diabetic foot ulcers?
The main cause is peripheral neuropathy, combined with poor blood circulation and impaired wound healing.
2. Why do diabetic foot ulcers heal slowly?
They heal slowly due to reduced blood flow, impaired immune response, and decreased growth factors.
3. Are diabetic foot ulcers painful?
Not always. Many are painless due to loss of sensation from neuropathy.
4. Can diabetic foot ulcers be prevented?
Yes, through proper foot care, good blood sugar control, and regular medical check-ups.
5. What is the most serious complication of DFU?
The most serious complication is amputation, often preceded by infection and tissue necrosis.