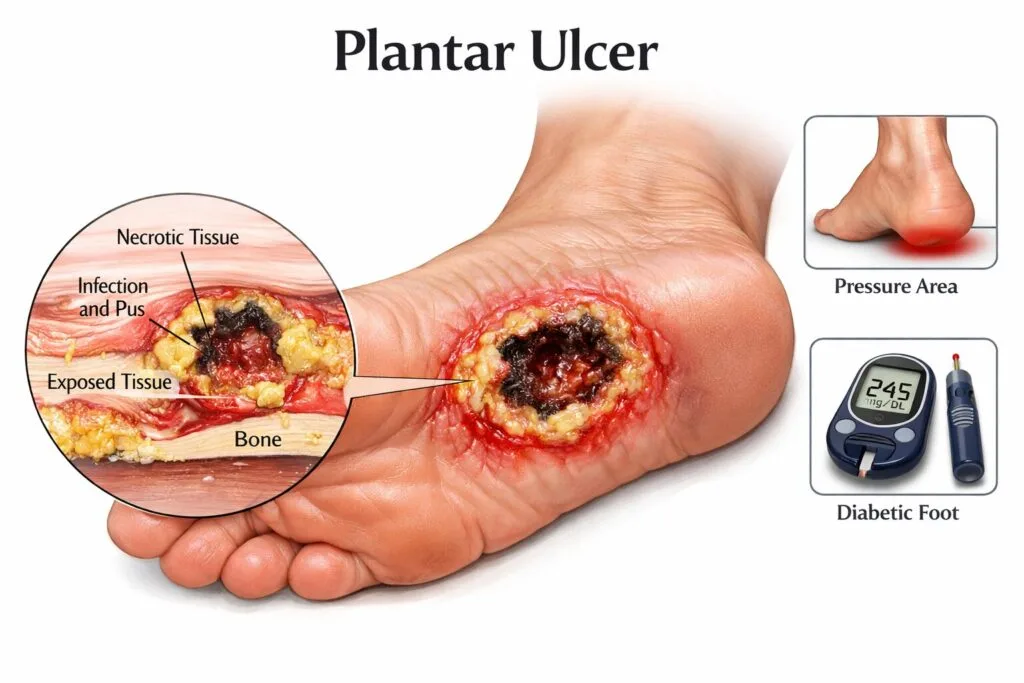
What Is a Plantar Ulcer? (And Why You Shouldn’t Ignore It)
A plantar ulcer is an open wound or sore that develops on the sole of the foot. If you or someone you care for has one, you already know it’s not just a minor inconvenience — left untreated, plantar ulcers can lead to serious infection, hospitalization, and in severe cases, amputation. The good news: with the right treatment plan and early action, most plantar ulcers can heal completely.
This guide covers everything you need to know — from the root causes and warning signs to the most effective treatments and prevention strategies.
What Causes Plantar Ulcers?
Plantar ulcers don’t appear overnight. They’re usually the result of sustained pressure, poor circulation, or nerve damage that prevents the body from protecting itself the way it normally would.
Diabetic Neuropathy
The most common cause of plantar ulcers is diabetic peripheral neuropathy — nerve damage that reduces sensation in the feet. When you can’t feel pain, a small blister or area of friction can quietly worsen into a deep wound before you ever notice it.
Prolonged Pressure and Friction
Standing or walking for long periods, ill-fitting shoes, or bony prominences (like bunions or hammertoes) can create concentrated pressure points on the sole of the foot. Over time, this repeated trauma breaks down the skin.
Poor Circulation (Peripheral Artery Disease)
Reduced blood flow means the tissues in the foot receive less oxygen and nutrients — both essential for healing. People with peripheral artery disease (PAD) are highly susceptible to wounds that simply won’t close.
Other Contributing Factors
- Obesity (increases load on foot structures)
- Kidney disease
- Previous history of foot ulcers
- Smoking (impairs circulation)
- Foot deformities
Signs and Symptoms to Watch For
Plantar ulcers can be deceptive — especially in people with reduced sensation. Here’s what to look for during routine foot checks:
Early Warning Signs
- Redness or discoloration on the sole
- Skin that feels warmer than surrounding areas
- Callus buildup around a central soft spot
- Mild swelling or firmness
Signs the Ulcer Has Progressed
- A visible open wound or crater on the foot
- Drainage, pus, or unusual odor
- Black or darkened tissue (a sign of tissue death)
- Fever or chills (may indicate systemic infection)
Important: Diabetics and those with nerve damage may feel no pain even with a severe ulcer. Daily visual inspection of both feet is non-negotiable.
How Are Plantar Ulcers Classified?
Healthcare providers use grading systems to assess severity. The most widely used is the Wagner Grading Scale:
| Grade | Description |
|---|---|
| 0 | No open lesion; high-risk foot |
| 1 | Superficial ulcer (skin only) |
| 2 | Deep ulcer to tendon, capsule, or bone |
| 3 | Deep ulcer with abscess or osteomyelitis |
| 4 | Partial foot gangrene |
| 5 | Full foot gangrene |
Grades 0–2 are generally managed with wound care and offloading. Grades 3 and above often require hospitalization and surgical intervention.
Plantar Ulcer Treatment: What Actually Works
Treatment is never one-size-fits-all. An effective plantar ulcer care plan addresses the wound itself, the underlying cause, and prevention of recurrence.
1. Offloading — The Single Most Important Step
Offloading means removing pressure from the ulcer site. Without it, even the best wound dressings will fail. Options include:
- Total Contact Cast (TCC): The gold standard. A custom cast distributes pressure evenly across the foot and limits movement.
- Removable Cast Walker (RCW): Easier to use than TCC but less effective if patients remove it frequently.
- Specialized footwear or insoles: Used for less severe ulcers or during the recovery phase.
2. Wound Debridement
Dead or infected tissue must be removed to allow healthy tissue to grow. A wound care specialist will clean the ulcer and remove necrotic material — a process called debridement. This may be done surgically, with specialized dressings, or via enzymatic agents.
3. Advanced Wound Dressings
Modern wound care has moved well beyond simple bandages. Common dressing types used for plantar ulcers include:
- Hydrocolloid dressings — maintain moist wound environment
- Foam dressings — absorb excess drainage
- Silver-impregnated dressings — antimicrobial for infected wounds
- Negative pressure wound therapy (NPWT) — uses gentle suction to promote healing in complex wounds
4. Infection Management
If the ulcer shows signs of infection, oral or intravenous antibiotics will be prescribed. Bone infections (osteomyelitis) require longer antibiotic courses and sometimes surgical bone removal.
5. Improving Blood Flow
For patients with PAD, restoring circulation is essential. Vascular surgeons may perform procedures such as angioplasty or bypass surgery to improve blood supply to the foot — dramatically improving healing outcomes.
6. Blood Sugar Control (for Diabetics)
High blood glucose impairs immune function and delays wound healing. Tight glycemic control during the healing phase is critical. Work closely with your endocrinologist or primary care physician to optimize blood sugar levels.
7. Surgical Options
In some cases, surgery is required to correct the underlying structural problem causing the ulcer — such as removing a bony prominence or correcting a foot deformity.
How Long Does a Plantar Ulcer Take to Heal?
Healing time depends on the ulcer’s depth, size, cause, and the patient’s overall health. Superficial ulcers in otherwise healthy individuals may close in a few weeks. Deeper wounds in diabetic or vascularly compromised patients can take several months — or may require surgical intervention.
Key factors that speed healing:
- Consistent offloading (wearing prescribed footwear every step)
- Good blood sugar control
- Adequate protein and nutrition
- No smoking
- Regular wound care appointments
Preventing Plantar Ulcers: Stop the Problem Before It Starts
For high-risk individuals, prevention is far better than treatment.
Daily Foot Care Habits
- Inspect feet every single day — use a mirror for the soles
- Wash feet with mild soap and lukewarm water; dry thoroughly between toes
- Moisturize (but not between toes, where moisture can cause fungal growth)
- Trim toenails straight across to avoid ingrown nails
Footwear Matters More Than You Think
- Always wear well-fitting shoes — never go barefoot, even indoors
- Look for shoes with extra depth and a wide toe box
- Consider custom orthotics if you have foot deformities or high pressure areas
- Check inside shoes before putting them on (foreign objects cause ulcers)
Regular Podiatry Visits
High-risk patients should see a podiatrist every 3 months — or more frequently if a wound is present or has recently healed. A podiatrist can identify pressure hotspots, manage calluses, and catch problems early.
FAQ
1. Can a plantar ulcer heal on its own without treatment?
Rarely, and it’s risky to try. Without offloading and proper wound care, plantar ulcers almost always worsen. What starts as a small wound can become deeply infected within days. Always seek professional care as soon as a wound is discovered.
2. Are plantar ulcers only a problem for diabetics?
No — while diabetics are at the highest risk, plantar ulcers can affect anyone with poor circulation, prolonged bed rest, nerve damage from other causes (such as spinal cord injury or chemotherapy), or significant foot deformities.
3. What does a plantar ulcer look like?
It typically appears as a round, punched-out wound on the ball of the foot or heel, sometimes surrounded by a ring of thickened callus. The wound bed may be pink (healthy), yellow (slough), or black (necrotic tissue).
4. Can plantar ulcers lead to amputation?
Yes — if left untreated or if infection spreads to the bone or bloodstream, amputation may become necessary to save the patient’s life. This is why early treatment is so critical. Studies show that up to 85% of diabetes-related amputations are preceded by a foot ulcer.
5. How do I know if my plantar ulcer is infected?
Signs of infection include increasing redness, warmth, swelling around the wound, pus or foul-smelling drainage, fever, and chills. If you notice any of these, seek medical care immediately — infected foot ulcers can progress to life-threatening sepsis within days.
Take the Next Step Toward Healing
Plantar ulcers are serious — but they’re treatable. The key is acting early, following a structured care plan, and working with the right specialists. Whether you’re managing a current wound or trying to protect at-risk feet, don’t wait for the problem to get worse.
Speak with a wound care specialist or podiatrist today. Early intervention is the most powerful tool you have. If you’re a diabetic or have risk factors for foot ulcers, schedule a preventive foot assessment — it could save your foot, and your life.